Blank Louisiana Medicaid Freedom of Choice List PDF Form
Blank Louisiana Medicaid Freedom of Choice List PDF Form
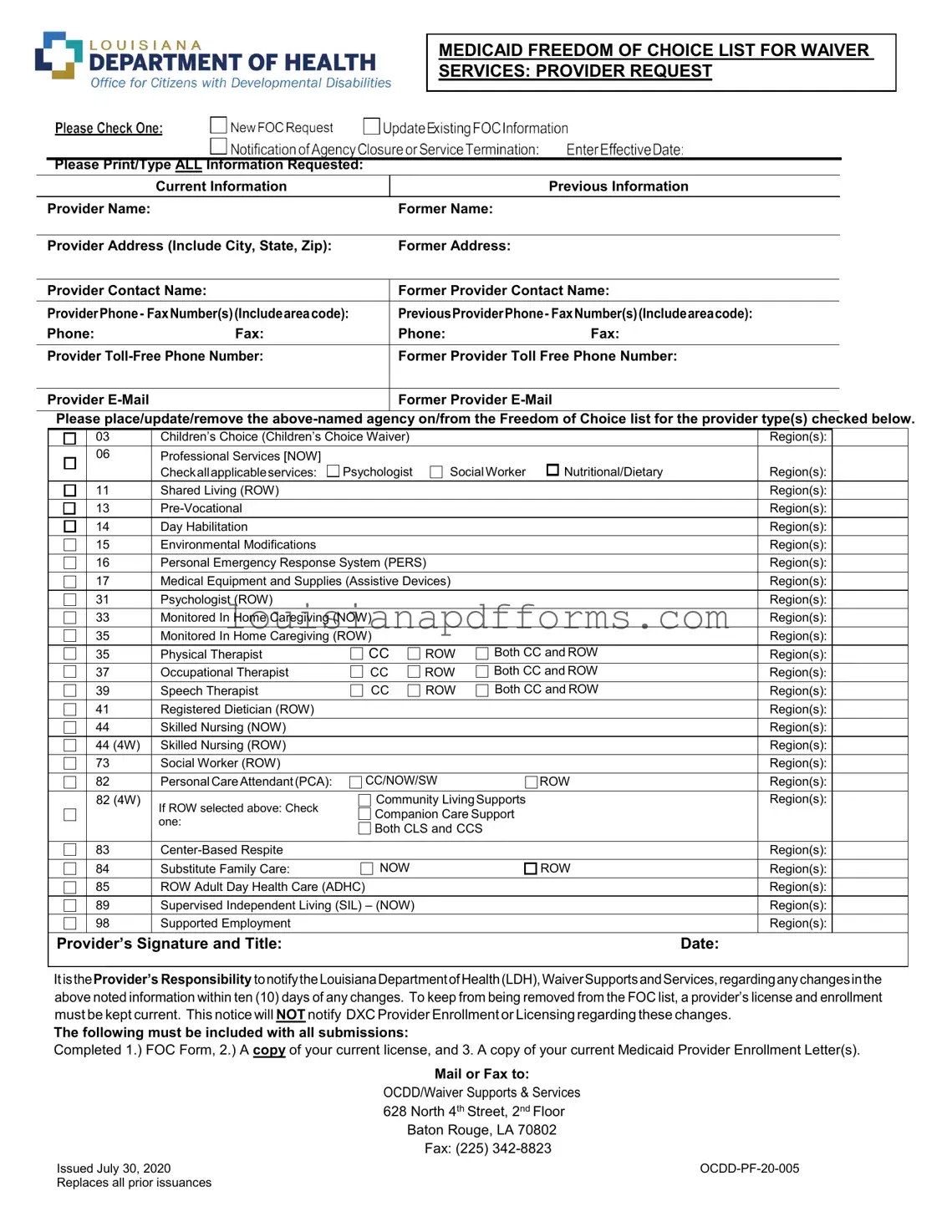
The Louisiana Medicaid Freedom of Choice List form is an essential document for providers offering waiver services within the state. This form facilitates the process of adding, updating, or removing agencies from the Freedom of Choice list, which is crucial for ensuring that individuals have access to necessary services. Providers must complete all requested information, including their current and former names, addresses, and contact details. A variety of service types are covered, such as Children’s Choice Waiver, Professional Services, and various therapeutic and supportive services. Each provider must check the applicable services and regions they wish to be listed under, ensuring that the information is accurate and comprehensive. Additionally, it is the provider's responsibility to notify the Louisiana Department of Health regarding any changes within ten days to maintain their standing on the list. To submit the form, providers must include a copy of their current license and Medicaid Provider Enrollment Letter, which reinforces their compliance with state regulations. This form is a key component in maintaining a network of qualified providers, thereby supporting the health and well-being of Medicaid recipients in Louisiana.
MEDICAID FREEDOM OF CHOICE LIST FOR WAIVER
SERVICES: PROVIDER REQUEST
Please Print/Type ALL Information Requested:
|
Current Information |
|
Previous Information |
|
|
|
|
Provider Name: |
|
Former Name: |
|
|
|
|
|
Provider Address (Include City, State, Zip): |
Former Address: |
|
|
|
|
||
Provider Contact Name: |
Former Provider Contact Name: |
||
|
|
||
ProviderPhone- FaxNumber(s)(Includeareacode): |
PreviousProviderPhone- FaxNumber(s)(Includeareacode): |
||
Phone: |
Fax: |
Phone: |
Fax: |
|
|
||
Provider |
Former Provider Toll Free Phone Number: |
||
|
|
|
|
Provider |
|
Former Provider |
|
|
|
|
|
Please place/update/remove the
|
03 |
Children’s Choice (Children’s Choice Waiver) |
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
|
06 |
Professional Services [NOW] |
|
|
|
|
|
|
|
|
|
Checkallapplicableservices: |
Psychologist |
SocialWorker |
Nutritional/Dietary |
|
Region(s): |
|
|
|
11 |
Shared Living (ROW) |
|
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
13 |
|
|
|
|
|
Region(s): |
|
|
|
14 |
Day Habilitation |
|
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
15 |
Environmental Modifications |
|
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
||
|
16 |
Personal Emergency Response System (PERS) |
|
|
|
Region(s): |
|
||
|
|
|
|
|
|
|
|
||
|
17 |
Medical Equipment and Supplies (Assistive Devices) |
|
|
|
Region(s): |
|
||
|
|
|
|
|
|
|
|
|
|
|
31 |
Psychologist (ROW) |
|
|
|
|
|
Region(s): |
|
|
33 |
Monitored In Home Caregiving (NOW) |
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
|
35 |
Monitored In Home Caregiving (ROW) |
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
|
35 |
Physical Therapist |
CC |
ROW |
Both CC and ROW |
|
Region(s): |
|
|
|
37 |
Occupational Therapist |
CC |
ROW |
Both CC and ROW |
|
: |
|
|
|
|
|
|
Region(s) |
|
||||
|
39 |
Speech Therapist |
CC |
ROW |
Both CC and ROW |
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
|
41 |
Registered Dietician (ROW) |
|
|
|
|
|
Region(s): |
|
|
44 |
Skilled Nursing (NOW) |
|
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
44 (4W) |
Skilled Nursing (ROW) |
|
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
73 |
Social Worker (ROW) |
|
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
82 |
Personal CareAttendant(PCA): |
CC/NOW/SW |
|
ROW |
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
||
|
82 (4W) |
If ROW selected above: Check |
Community LivingSupports |
|
|
Region(s): |
|
||
|
|
Companion Care Support |
|
|
|
|
|||
|
|
one: |
|
|
|
|
|||
|
|
Both CLS and CCS |
|
|
|
|
|
||
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
83 |
|
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
|
84 |
Substitute Family Care: |
NOW |
|
|
ROW |
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
85 |
ROW Adult Day Health Care (ADHC) |
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
|
89 |
Supervised Independent Living (SIL) – (NOW) |
|
|
|
|
Region(s): |
|
|
|
98 |
Supported Employment |
|
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
Provider’s Signature and Title: |
|
|
|
|
Date: |
||||
|
|
|
|
|
|
|
|
|
|
ItistheProvider’s Responsibility tonotifytheLouisianaDepartmentofHealth(LDH),WaiverSupportsandServices,regardinganychangesinthe above noted information within ten (10) days of any changes. To keep from being removed from the FOC list, a provider’s license and enrollment must be kept current. This notice will NOT notify DXC Provider Enrollment or Licensing regarding these changes.
The following must be included with all submissions:
Completed 1.) FOC Form, 2.) A copy of your current license, and 3. A copy of your current Medicaid Provider Enrollment Letter(s).
Mail or Fax to:
OCDD/Waiver Supports & Services
628North 4th Street, 2nd Floor Baton Rouge, LA 70802 Fax: (225)
Issued July 30, 2020 |
|
Replaces all prior issuances |
|
When filling out the Louisiana Medicaid Freedom of Choice List form, it is crucial to follow specific guidelines to ensure accuracy and compliance. Below is a list of recommendations on what to do and what to avoid.
Road Tax for Commercial Vehicles - Retention of records related to this application is often recommended for applicants.
A Durable Power of Attorney (DPOA) is a legal document that allows you to designate someone to make decisions on your behalf if you become incapacitated. In Arizona, this form is essential for ensuring your financial and medical matters are handled according to your wishes. For more information and a template to help you create this important document, visit https://arizonapdfs.com/durable-power-of-attorney-template/. Understanding how to properly complete and execute this document is crucial for protecting your interests.
Louisiana Amended Tax Return - Students should ensure their requests are complete to avoid processing issues.
Dpsmv 1606 - Submitting this form accurately can simplify the registration process for the buyer.
Completing the Louisiana Medicaid Freedom of Choice List form is an important step in ensuring that your provider information is accurately recorded. After filling out the form, you will need to submit it along with the required documents to the appropriate department. This will help maintain your provider's status on the Freedom of Choice list and ensure compliance with Medicaid requirements.
The Louisiana Medicaid Freedom of Choice List form is essential for providers offering waiver services. However, several other documents often accompany this form to ensure compliance and proper processing. Below is a list of these documents, along with a brief description of each.
Each of these documents plays a crucial role in the process of providing Medicaid services in Louisiana. Having them ready and properly filled out can help ensure a smooth experience for both providers and clients.
The Louisiana Medicaid Freedom of Choice List form is a document used by providers to request inclusion, update, or removal from the Freedom of Choice list for waiver services. This form is essential for ensuring that providers are correctly listed for the services they offer under Medicaid.
Providers of waiver services under Louisiana Medicaid must complete this form. This includes various types of service providers such as psychologists, social workers, and personal care attendants, among others. It is crucial for maintaining accurate records and ensuring that eligible individuals can access the necessary services.
The form requires both current and previous information about the provider. This includes:
Additionally, providers must indicate the specific services they offer and the regions in which they operate.
Once the form is completed, it can be submitted by mail or fax. The mailing address is:
OCDD/Waiver Supports & Services
628 North 4th Street, 2nd Floor
Baton Rouge, LA 70802
The fax number for submissions is (225) 342-8823.
Providers must include the following documents when submitting the form:
If a provider fails to notify the Louisiana Department of Health about any changes within ten days, they may be removed from the Freedom of Choice list. It is the provider's responsibility to ensure that their license and enrollment remain current to avoid removal.
This version of the form was issued on July 30, 2020, and it replaces all prior issuances. Providers should ensure they are using the most current form to avoid issues with their submissions.
Filling out the Louisiana Medicaid Freedom of Choice List form can be straightforward, but mistakes can lead to delays or complications. One common error is not providing current information. Applicants often list outdated addresses or contact details. This can cause confusion and prevent timely communication between the provider and the Louisiana Department of Health. Always double-check that the information is accurate and up to date.
Another frequent mistake is failing to include all necessary documentation. The form requires a copy of the current license and the Medicaid Provider Enrollment Letter. Without these documents, the submission may be incomplete. This can lead to rejection or further requests for information, which can slow down the process significantly.
People sometimes neglect to check all applicable services. The form has specific sections where providers must indicate the types of services they offer. Omitting a service or failing to mark the correct regions can result in providers being excluded from the Freedom of Choice list. It’s essential to review the services thoroughly to ensure everything is accurately represented.
Lastly, some applicants overlook the importance of the provider’s signature and date. This final step is crucial for validating the form. Without a signature, the submission may not be considered official, leading to further delays. Always remember to sign and date the form before sending it in.
Here are nine misconceptions about the Louisiana Medicaid Freedom of Choice List form, along with clarifications for each:
| Fact Name | Description |
|---|---|
| Purpose of the Form | The Louisiana Medicaid Freedom of Choice List form is used by providers to request inclusion or updates to the Freedom of Choice list for waiver services. |
| Required Information | Providers must provide current and previous information, including names, addresses, contact details, and phone numbers. |
| Services Covered | The form covers a variety of services, such as psychological services, personal care attendants, and skilled nursing, among others. |
| Governing Laws | This form is governed by Louisiana Medicaid regulations, specifically under the Louisiana Department of Health guidelines for waiver services. |
| Submission Requirements | Providers must submit the completed form along with a current license and Medicaid Provider Enrollment Letter to the designated office. |
| Notification Responsibility | It is the provider's responsibility to notify the Louisiana Department of Health of any changes within ten days to maintain their status on the list. |