Blank Medical Examination Louisiana PDF Form
Blank Medical Examination Louisiana PDF Form
The Medical Examination Louisiana form is an essential document required by the Louisiana Department of Public Safety and Corrections for individuals applying for or renewing their driver’s licenses. This form mandates that applicants undergo a medical evaluation by a licensed physician, who will assess various health factors that may impact the applicant's ability to operate a vehicle safely. The examination covers a wide range of areas, including the applicant's medical history, vision, hearing, neurological and cardiovascular health, as well as any mental health considerations. It is crucial for the physician to complete the form thoroughly, as any incomplete sections may lead to the denial of the applicant's driving privileges. Additionally, the form must be submitted within 30 days of issuance to avoid suspension of driving rights. The physician is also protected from liability when reporting any medical conditions that could impair driving abilities, ensuring that the evaluation process prioritizes public safety. By carefully documenting the applicant's health status, this form serves as a vital tool in determining fitness to drive, reflecting the state's commitment to ensuring safe roads for all.
LOUISIANA DEPARTMENT OF PUBLIC SAFETY & CORRECTIONS
OFFICE OF MOTOR VEHICLES
MEDICAL EXAMINATION FORM
P. O. BOX 64886 • BATON ROUGE, LA
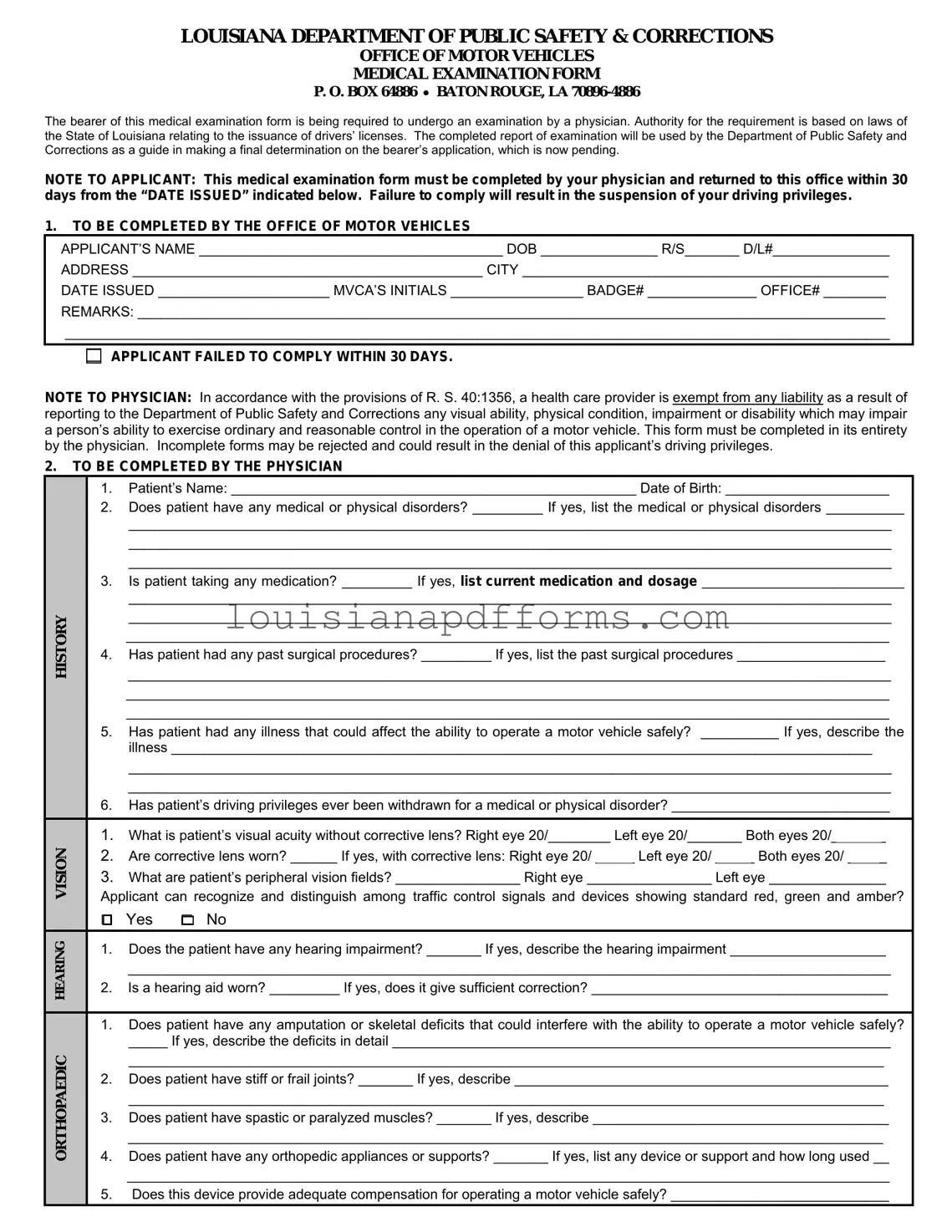
The bearer of this medical examination form is being required to undergo an examination by a physician. Authority for the requirement is based on laws of the State of Louisiana relating to the issuance of drivers’ licenses. The completed report of examination will be used by the Department of Public Safety and Corrections as a guide in making a final determination on the bearer’s application, which is now pending.
NOTE TO APPLICANT: This medical examination form must be completed by your physician and returned to this office within 30 days from the “DATE ISSUED” indicated below. Failure to comply will result in the suspension of your driving privileges.
1.TO BE COMPLETED BY THE OFFICE OF MOTOR VEHICLES
APPLICANT’S NAME _______________________________________ DOB _______________ R/S_______ D/L#_______________
ADDRESS _____________________________________________ CITY _______________________________________________
DATE ISSUED ______________________ MVCA’S INITIALS _________________ BADGE# ______________ OFFICE# ________
REMARKS: ________________________________________________________________________________________________
__________________________________________________________________________________________________________
APPLICANT FAILED TO COMPLY WITHIN 30 DAYS.
NOTE TO PHYSICIAN: In accordance with the provisions of R. S. 40:1356, a health care provider is exempt from any liability as a result of reporting to the Department of Public Safety and Corrections any visual ability, physical condition, impairment or disability which may impair a person’s ability to exercise ordinary and reasonable control in the operation of a motor vehicle. This form must be completed in its entirety by the physician. Incomplete forms may be rejected and could result in the denial of this applicant’s driving privileges.
2.TO BE COMPLETED BY THE PHYSICIAN
HISTORY
ORTHOPAEDIC HEARING VISION
1.Patient’s Name: ____________________________________________________ Date of Birth: _____________________
2.Does patient have any medical or physical disorders? _________ If yes, list the medical or physical disorders __________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
3.Is patient taking any medication? _________ If yes, list current medication and dosage __________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
4.Has patient had any past surgical procedures? _________ If yes, list the past surgical procedures ___________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
5.Has patient had any illness that could affect the ability to operate a motor vehicle safely? __________ If yes, describe the illness __________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
6.Has patient’s driving privileges ever been withdrawn for a medical or physical disorder? ____________________________
1.What is patient’s visual acuity without corrective lens? Right eye 20/________ Left eye 20/_______ Both eyes 20/_______
2.Are corrective lens worn? ______ If yes, with corrective lens: Right eye 20/ _____ Left eye 20/ _____ Both eyes 20/ _____
3.What are patient’s peripheral vision fields? ________________ Right eye ________________ Left eye _______________
Applicant can recognize and distinguish among traffic control signals and devices showing standard red, green and amber?
□ Yes □ No
1.Does the patient have any hearing impairment? _______ If yes, describe the hearing impairment ____________________
__________________________________________________________________________________________________
2.Is a hearing aid worn? _________ If yes, does it give sufficient correction? ______________________________________
1.Does patient have any amputation or skeletal deficits that could interfere with the ability to operate a motor vehicle safely?
_____ If yes, describe the deficits in detail ________________________________________________________________
_________________________________________________________________________________________________
2.Does patient have stiff or frail joints? _______ If yes, describe ________________________________________________
_________________________________________________________________________________________________
3.Does patient have spastic or paralyzed muscles? _______ If yes, describe ______________________________________
_________________________________________________________________________________________________
4.Does patient have any orthopedic appliances or supports? _______ If yes, list any device or support and how long used __
__________________________________________________________________________________________________
5.Does this device provide adequate compensation for operating a motor vehicle safely? ____________________________
NEUROLOGICAL CARDIOPULMONARY
MENTAL
DIABETES
3.
1.Does patient have angina?______ If yes, when does it occur?_____strenuous activity_____normal activity_____at rest_____
2.Does patient have dyspnea?_____If yes, when does it occur?_____strenuous activity_____normal activity_____at rest_____
3.Does patient have syncope?_____if yes, what is the frequency?__________duration___________last occurance_________
4.Does patient have dizziness?______ describe______________________________________________________________
___________________________________________________________________________________________________
5.What is patient’s blood pressure? 1st reading __________________________ 2nd reading __________________________
6.What is patient’s pulse? Rate __________________________________ Rhythm __________________________________
7.Has patient had cardiovascular catheterization or surgery? ______ If yes, describe _________________________________
___________________________________________________________________________________________________
List medications and dosage: ____________________________________________________________________________
1.Does patient have epilepsy? ______If yes, what type of seizures? _________________ Date of last seizure? ____________
Are seizures completely controlled? _______ Is patient under regular medical care? ________________________________
What are the anticonvulsant serum blood levels? ____________________________________________________________
2.Does patient have any signs of Parkinsonism? ______ If yes, describe condition and severity _________________________
___________________________________________________________________________________________________
Is coordination normal? _______ If no, describe _____________________________________________________________
3.Does patient have any neurological disorder? ______ If yes, describe ___________________________________________
List medications and dosage: ____________________________________________________________________________
Is patient reliable in taking medication and following medical regimen? _____________________________________________
1.Does patient have symptoms of any mental disorder? ______ If yes, describe condition and severity at present ___________
___________________________________________________________________________________________________
2.Has patient ever been treated in a mental hospital? _______ If yes, where and when _______________________________
What was diagnosis and cure? __________________________________________________________________________
3.Does patient use alcohol or drugs? ______ If yes, describe usage ______________________________________________
4.Is patient mentally deficient? ______ If yes, what was highest grade attained in school? ________ age at attainment? _____
5.Does patient have sufficient regard for his/her personal safety as well as that of others to operate a motor vehicle safely? Give details _________________________________________________________________________________________
6.Is patient likely to act on sudden impulse without regard for the consequences of his/her behavior? ____________________
Give details _________________________________________________________________________________________
7.On the basis of your examination and/or knowledge of this patient, do you recommend periodic psychiatric examinations? Give details _________________________________________________________________________________________
List medications and dosage: ____________________________________________________________________________
1.Does patient have a history of diabetes? _______ If yes, is insulin taken? ______ is oral medication taken? ______________
2.What are patient’s laboratory studies? recent urine sugars __________________ recent blood sugars __________________
3.Has patient had any occurrences of diabetic coma? ________ If yes, give dates ___________________________________
4.Has patient had any occurrences of insulin shock? ________ If yes, give dates ____________________________________
5.Does patient have associated abnormalities? visual_______renal_______vascular_______neurological_______other______ If yes, describe _______________________________________________________________________________________
6.Does patient have hypoglycemia? _______ If yes, describe treatment ___________________________________________
List medications taken and dosage: _______________________________________________________________________
Is patient reliable in taking diabetes medication? ______________________ Is diabetes controlled? ______________________
TO BE SIGNED BY PATIENT
I hereby authorize the examining physician whose signature appears below to release all information and findings contained herein to the Louisiana Department of Public Safety and Corrections. The Louisiana Department of Public Safety and Corrections can release this information to such individuals or groups as may be considered necessary and appropriate to determine my ability to safely operate a motor vehicle.
Date _____________________________________ |
Signature of Patient _______________________________________________________ |
4.TO BE COMPLETED, SIGNED AND DATED BY THE PHYSICIAN
PLEASE REFER TO “NOTE TO PHYSICIAN:” on the first page of this form. Are you this patient’s treating physician? _____________
In your opinion, from a medical standpoint, is it safe for this patient to operate a motor vehicle? _______________________________
On the basis of your examination and/or knowledge of this patient, do you recommend periodic medical reports be submitted? _______
If yes, how often? |
6 months |
1 year |
2 years |
other__________ Remarks: ________________________________ |
___________________________________________________________________________________________________________ |
||||
Physician’s Signature _________________________________________________________ Date ___________________________
Physician’s Printed Name ______________________________________________________ Telephone# _____________________
Physician’s Address __________________________________________________________________________________________
DPSMV 2032 (R 04/04)
When filling out the Medical Examination Louisiana form, it is important to follow specific guidelines to ensure the process goes smoothly. Below are seven recommendations regarding what to do and what to avoid.
Petition to Establish Paternity Louisiana - Requires mutual consent if the mother has a husband or ex-husband.
For those looking to understand the intricacies of a thorough Residential Lease Agreement process, this form will guide you through the necessary steps, ensuring both landlords and tenants are well-informed of their rights and obligations throughout the rental period.
Deq 641 581Cert - The form requires a work order number for tracking purposes.
Completing the Medical Examination Louisiana form is essential for your driving privileges. After you fill out the necessary sections, your physician will conduct an examination and provide their findings. Ensure that the completed form is submitted within 30 days to avoid any suspension of your driving privileges.
The Medical Examination Louisiana form is an essential document required for individuals applying for or renewing their driver's licenses in Louisiana. However, it is often accompanied by several other forms and documents that help provide a comprehensive view of the applicant's health and driving capabilities. Here’s a brief overview of six commonly used documents that may accompany the Medical Examination form.
Each of these forms plays a crucial role in ensuring that individuals are medically fit to drive, thereby promoting safety on the roads. Understanding these documents can help applicants navigate the process more smoothly and enhance their chances of obtaining or retaining their driving privileges.
The Medical Examination Louisiana form is required for individuals applying for a driver's license in Louisiana. It serves as a means for the Department of Public Safety and Corrections to assess the applicant's medical fitness to operate a motor vehicle. The completed form provides crucial information about the applicant's health, which aids in determining whether they can safely drive.
The form must be completed by a licensed physician. It is essential that the physician provides thorough and accurate information regarding the applicant's medical history, current health status, and any conditions that may affect their ability to drive safely.
If the completed form is not returned to the Office of Motor Vehicles within 30 days from the date issued, the applicant's driving privileges will be suspended. Timely submission is crucial to avoid any interruptions in driving rights.
The physician must provide detailed information regarding:
Incomplete forms may be rejected, which could jeopardize the applicant's ability to obtain a driver's license.
If an applicant has a medical condition that could affect their driving ability, it is vital to disclose this information to the physician. The physician will assess the condition and determine whether it poses a risk when operating a vehicle. Full transparency is essential for ensuring safety on the roads.
No, physicians are exempt from liability when reporting a patient's medical condition that may impair their ability to drive. This protection allows healthcare providers to fulfill their duty to ensure public safety without fear of legal repercussions.
The physician must sign and date the form to validate it. Additionally, they should print their name and provide their contact information. This ensures that the Office of Motor Vehicles can reach out if further information is needed.
If an applicant disagrees with the physician's assessment regarding their ability to drive, they should discuss their concerns directly with the physician. It may also be possible to seek a second opinion from another qualified medical professional. However, the final determination will be made by the Department of Public Safety and Corrections based on the submitted medical information.
Completing the Medical Examination Louisiana form can be a straightforward process, but several common mistakes can lead to delays or complications. One frequent error occurs when applicants fail to provide their full name and date of birth accurately. This information is crucial for identifying the individual and linking the examination results to the correct application. A simple misspelling or omission can cause significant issues.
Another mistake is not adhering to the 30-day submission deadline. The form must be completed by a physician and returned to the Office of Motor Vehicles within this timeframe. If applicants overlook this requirement, they risk having their driving privileges suspended. It’s essential to keep track of the date issued and plan accordingly.
Many applicants also neglect to ensure that the physician fills out the form completely. Incomplete forms may be rejected, which can lead to delays in processing the application. Each section of the form is designed to gather specific information about the applicant’s health, and missing details can hinder the evaluation process.
Inaccuracies in reporting medical history represent another common pitfall. When answering questions about medical or physical disorders, medications, and past surgeries, it’s vital to provide thorough and truthful information. Inconsistencies can raise red flags and may result in the denial of driving privileges.
Applicants often forget to indicate whether they wear corrective lenses. This detail is critical for assessing visual acuity and overall safety while driving. If a patient does wear corrective lenses, the form must reflect their vision with and without these aids accurately.
Another area where mistakes frequently occur is in the section regarding hearing impairments. Applicants sometimes fail to mention the use of hearing aids or other assistive devices. If applicable, detailing the effectiveness of these aids is equally important, as it impacts the overall assessment of the applicant's ability to drive safely.
In the neurological section, individuals may overlook disclosing relevant conditions or medications. This oversight can be particularly concerning if the applicant has a history of seizures or other neurological disorders. Full disclosure helps ensure that the physician can make an informed recommendation regarding the applicant's ability to operate a vehicle.
Applicants sometimes forget to sign the form, which can lead to delays in processing. The signature of the patient is required to authorize the release of medical information to the Department of Public Safety and Corrections. Without this signature, the form cannot be considered valid.
Additionally, the physician must also complete and sign their section of the form. If this step is skipped, the entire application could be rejected. Physicians should carefully review their notes and ensure all questions are answered thoroughly and accurately.
Lastly, applicants may fail to keep a copy of the completed form for their records. Having a copy can be beneficial if any questions arise later regarding the submitted information. It serves as a reference point and can help clarify any potential misunderstandings.
Misconceptions about the Medical Examination Louisiana form can lead to confusion and potential issues for applicants. Here are seven common misunderstandings:
| Fact Name | Details |
|---|---|
| Governing Laws | The medical examination form is governed by Louisiana Revised Statutes (R.S.) 40:1356. |
| Purpose of the Form | This form is required for individuals applying for a driver's license to ensure they meet medical standards. |
| Submission Deadline | The completed form must be returned within 30 days from the date issued to avoid suspension of driving privileges. |
| Physician's Responsibility | The physician must complete the form entirely; incomplete forms may lead to denial of the applicant's driving privileges. |
| Visual Acuity Assessment | The form requires the physician to evaluate the patient's visual acuity with and without corrective lenses. |
| Hearing Impairment Evaluation | Physicians must assess any hearing impairments and whether corrective devices are used. |
| Medical History | Applicants must disclose any medical or physical disorders that could affect their ability to drive safely. |
| Signatures Required | Both the patient and the physician must sign the form to authorize the release of medical information. |
| Periodic Medical Reports | Physicians may recommend periodic medical reports based on their examination of the patient. |
| Liability Exemption | Under R.S. 40:1356, healthcare providers are exempt from liability when reporting medical conditions affecting driving ability. |