Blank State Of Louisiana Medication Order PDF Form
Blank State Of Louisiana Medication Order PDF Form
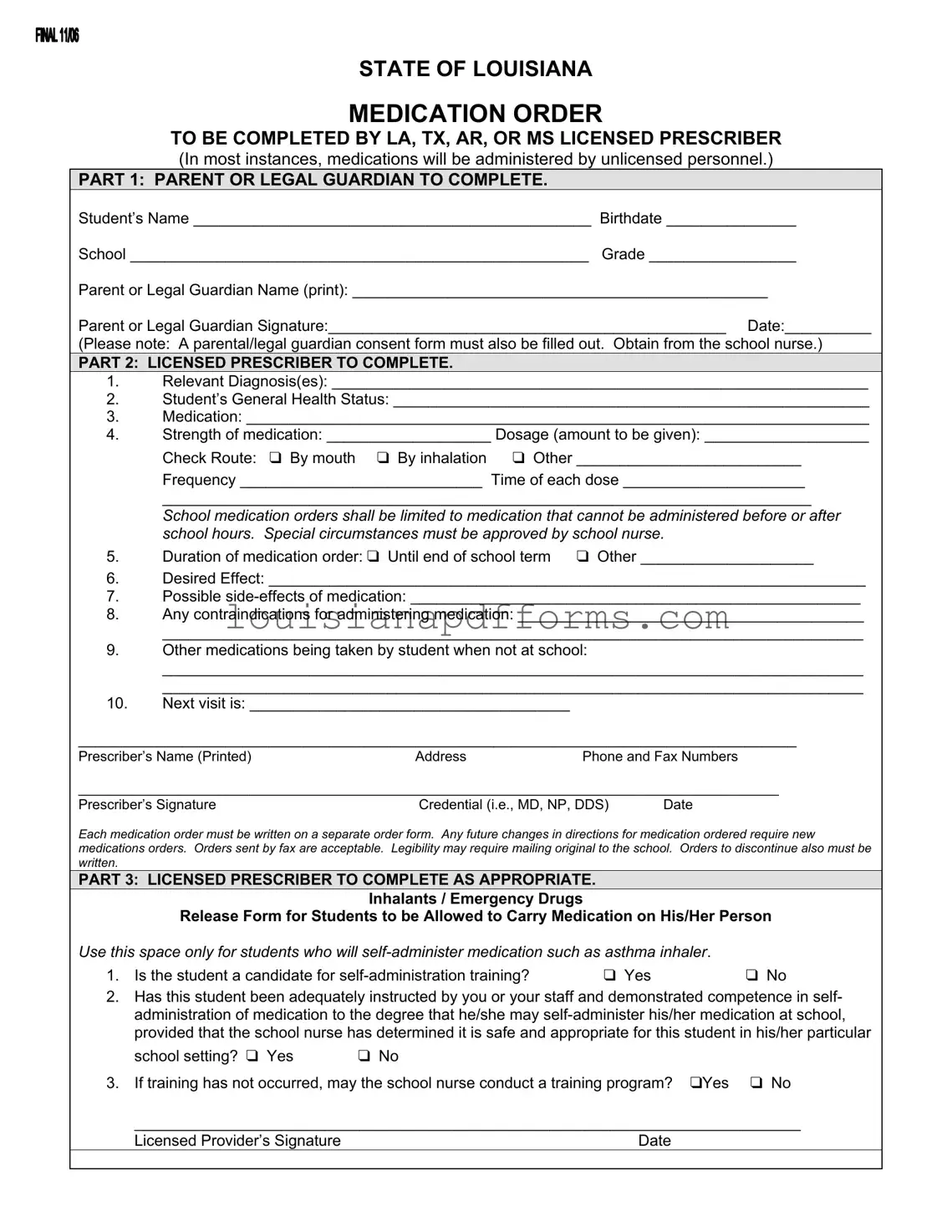
The State of Louisiana Medication Order form serves as a crucial document for ensuring that students who require medication during school hours receive the appropriate care. Designed to be completed by licensed prescribers from Louisiana, Texas, Arkansas, or Mississippi, this form is structured in three distinct parts, each serving a specific purpose. The first section is dedicated to the parent or legal guardian, who must provide essential information about the student, including their name, birthdate, and school details. This section also requires the guardian's signature, affirming consent for the medication administration. In the second part, the licensed prescriber outlines vital information such as the student’s diagnosis, general health status, and specific medication details, including dosage, frequency, and route of administration. It is important to note that the form limits medication orders to those that cannot be given before or after school, ensuring that all protocols are followed for the student’s safety. Additionally, the prescriber must indicate any potential side effects and contraindications, as well as other medications the student may be taking outside of school. The third part addresses special circumstances, allowing for students to self-administer certain medications, like inhalers, under specific conditions. This comprehensive approach not only safeguards the well-being of students but also facilitates clear communication among parents, healthcare providers, and school staff.
STATE OF LOUISIANA
MEDICATION ORDER
TO BE COMPLETED BY LA, TX, AR, OR MS LICENSED PRESCRIBER
(In most instances, medications will be administered by unlicensed personnel.)
PART 1: PARENT OR LEGAL GUARDIAN TO COMPLETE.
Student’s Name ______________________________________________ Birthdate _______________
School _____________________________________________________ Grade _________________
Parent or Legal Guardian Name (print): ________________________________________________
Parent or Legal Guardian Signature:______________________________________________ Date:__________
(Please note: A parental/legal guardian consent form must also be filled out. Obtain from the school nurse.)
PART 2: LICENSED PRESCRIBER TO COMPLETE.
1.Relevant Diagnosis(es): ______________________________________________________________
2.Student’s General Health Status: _______________________________________________________
3.Medication: ________________________________________________________________________
4.Strength of medication: ___________________ Dosage (amount to be given): ___________________
|
Check Route: ❑ By mouth ❑ By inhalation ❑ Other __________________________ |
|
|
Frequency ____________________________ Time of each dose _____________________ |
|
|
___________________________________________________________________________ |
|
|
School medication orders shall be limited to medication that cannot be administered before or after |
|
|
school hours. Special circumstances must be approved by school nurse. |
|
5. |
Duration of medication order: ❑ Until end of school term |
❑ Other ____________________ |
6.Desired Effect: _____________________________________________________________________
7.Possible
8.Any contraindications for administering medication: ________________________________________
_________________________________________________________________________________
9.Other medications being taken by student when not at school:
_________________________________________________________________________________
_________________________________________________________________________________
10.Next visit is: _____________________________________
___________________________________________________________________________________
Prescriber’s Name (Printed)AddressPhone and Fax Numbers
__________________________________________________________________________________________
Prescriber’s Signature |
Credential (i.e., MD, NP, DDS) |
Date |
Each medication order must be written on a separate order form. Any future changes in directions for medication ordered require new medications orders. Orders sent by fax are acceptable. Legibility may require mailing original to the school. Orders to discontinue also must be written.
PART 3: LICENSED PRESCRIBER TO COMPLETE AS APPROPRIATE.
Inhalants / Emergency Drugs
Release Form for Students to be Allowed to Carry Medication on His/Her Person
Use this space only for students who will |
|
|
1. Is the student a candidate for |
❑ Yes |
❑ No |
2.Has this student been adequately instructed by you or your staff and demonstrated competence in self- administration of medication to the degree that he/she may
school setting? ❑ Yes ❑ No
3. If training has not occurred, may the school nurse conduct a training program? ❑Yes ❑ No
_____________________________________________________________________________
Licensed Provider’s Signature |
Date |
When filling out the State of Louisiana Medication Order form, it’s crucial to ensure accuracy and compliance with guidelines. Here’s a list of things you should and shouldn’t do:
Warranty Deed Louisiana - It provides legal clarity concerning the family home designation.
In order to facilitate the transfer of ownership and avoid any ambiguities, it is recommended to utilize an accurate and legally recognized form, such as the one available at Fast PDF Templates, ensuring all necessary details are captured effectively.
R-1310 - Dealers must maintain records of their exemption claims for auditing purposes.
What Do I Need for New Car Registration - There are specific deadlines mentioned for submitting the application to avoid penalties.
Filling out the State of Louisiana Medication Order form is a crucial step in ensuring that a student receives the necessary medication during school hours. This process involves multiple parties, including parents or legal guardians and licensed prescribers. To accurately complete the form, follow the steps outlined below.
The State of Louisiana Medication Order form is an essential document for managing student medications in schools. Alongside this form, several other documents may be necessary to ensure proper medication administration and compliance with regulations. Below is a list of related forms that are commonly used.
Understanding these forms and their purposes can help streamline the process of managing student medications effectively. Proper documentation ensures that students receive the necessary care while at school.
The Louisiana Medication Order form is used to ensure that students receive their prescribed medications during school hours. It is designed to be filled out by both a parent or legal guardian and a licensed prescriber. This form helps schools manage medication administration safely and effectively.
The form consists of three parts:
The parent or legal guardian must provide the following details:
Additionally, they must complete a parental consent form, which can be obtained from the school nurse.
The licensed prescriber must provide detailed information about the student’s diagnosis, health status, medication, dosage, frequency, and any possible side effects. They also need to indicate the duration of the medication order and any other medications the student is taking.
No, the school medication orders are limited to medications that cannot be given before or after school hours. If there are special circumstances, these must be approved by the school nurse.
If there are any changes in the directions for the medication, a new medication order must be written. Each medication order should be on a separate form. Orders can be sent by fax, but the original may need to be mailed for legibility.
Filling out the State of Louisiana Medication Order form can be straightforward, but several common mistakes can lead to delays or complications. One significant error is failing to provide complete information in the Student’s Name and Birthdate sections. Omitting any part of this information can cause confusion and hinder the medication administration process. It is essential to ensure that the student’s name is spelled correctly and that the birthdate matches the records.
Another frequent mistake occurs when parents or legal guardians neglect to sign the form. The Parent or Legal Guardian Signature is a critical component of the document. Without it, the school cannot proceed with administering the medication. Additionally, the date of the signature must be included. Missing this detail can lead to misunderstandings about when consent was granted.
Inaccuracies in the Medication section can also pose serious risks. Parents must ensure that the medication name is correct and that the dosage is clearly indicated. Ambiguities in this section can lead to misadministration, which may endanger the student's health. It is crucial to double-check that the strength of the medication and the dosage match the prescriber's instructions.
Another common oversight is neglecting to specify the Route of administration. The form provides options such as "By mouth" or "By inhalation," and it is vital to check the appropriate box. Failing to do so can result in the medication being administered incorrectly. Furthermore, the Frequency and Time of each dose must be clearly stated to ensure that the medication is given as prescribed.
Lastly, individuals often overlook the requirement for a separate order form for each medication. If multiple medications are needed, each must be documented on its own form. Additionally, any changes in medication directions require new orders. This oversight can create confusion and disrupt the medication regimen. Always ensure that each medication order is submitted correctly and promptly.
1. The form can be completed by anyone. This is incorrect. Only licensed prescribers from Louisiana, Texas, Arkansas, or Mississippi can fill out the medication order form. It is essential that a qualified professional assesses the student’s health needs.
2. Medications can be administered at any time during school hours. This misconception arises from a misunderstanding of the rules. Medications listed on this form can only be given during school hours if they cannot be taken before or after school. Special cases must be approved by the school nurse.
3. Parents do not need to sign anything. Parents or legal guardians must complete and sign the first part of the form. This signature is crucial as it provides consent for the medication to be administered to the student.
4. One medication order form can cover multiple medications. Each medication must have its own separate order form. This ensures clarity and proper documentation for each medication the student is taking.
5. Faxed orders are not acceptable. In fact, faxed orders are permitted. However, if legibility is an issue, the original order may need to be mailed to the school. Clarity in the order is essential for safe administration.
6. The form is only for long-term medication. This is a common misunderstanding. The form can be used for both short-term and long-term medications, but the duration must be specified by the prescriber.
7. The school nurse has no role in the medication administration process. This is false. The school nurse plays a vital role in approving special circumstances and ensuring that medications are administered safely and appropriately. Their expertise is crucial in managing student health needs.
| Fact Name | Details |
|---|---|
| Governing Law | The medication order form is governed by Louisiana Revised Statutes, Title 17, Section 436.1. |
| Intended Users | This form is to be completed by licensed prescribers from Louisiana, Texas, Arkansas, or Mississippi. |
| Parental Involvement | A parent or legal guardian must complete the first part of the form, providing necessary information and consent. |
| Medication Administration | In most cases, medications will be administered by unlicensed personnel under the supervision of a school nurse. |
| Medication Restrictions | School medication orders are limited to medications that cannot be given before or after school hours. |
| Self-Administration | Students may be allowed to carry certain medications, like inhalers, if they meet specific criteria set by the prescriber and school nurse. |
| Separate Orders | Each medication order must be written on a separate form. Changes require new orders. |
| Fax Orders | Orders can be sent by fax, but original copies may need to be mailed for legibility. |